Older adults in Wales who had the jab were 20% less likely to be diagnosed with dementia that those not vaccinated
This week a new study published in Nature added to the evidence that getting a vaccine vs Shingles (Herpes Zoster) reduces the subsequent risk of dementia. It is the most rigorous study performed to date, but still leaves us with many questions. In this edition of Ground Truths, I will review the new report and previous ones for this vaccine and others, to address the following questions:
- Do the Shingle vaccines (Zostavax, the live attenuated virus, no longer available, and Shingrix, the recombinant vaccine) reduce the risk of dementia?
- Is this effect for reducing Alzheimer’s disease or dementia?
- What is the mechanism of the benefit?
Is the Risk of Dementia Reduced?
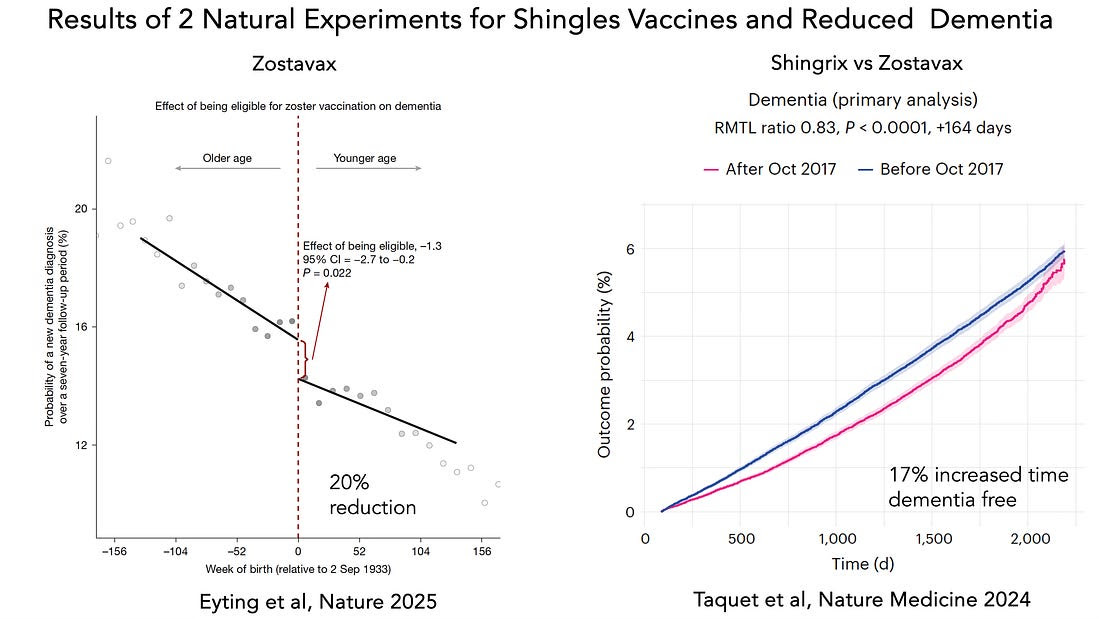
Until recently, the studies looking at this question were observational, retrospective, and plagued by multiple confounding factors. There are now 2 natural experiments (naturally occurring events) based on polices for vaccine eligibility or their receipt. The first of these was published in 2024 in Nature Medicine that was afforded by the rapid switch in the United States from Zostavax to Shingrix (right panel below). The latter was associated with a 17% increase in freedom from a dementia diagnosis. The new study (left panel below) based upon Zostavax vaccine eligibility by a cutoff birth date in Wales which resulted in 47% (eligible) vs 0% (for ineligible) vaccinated and a 20% reduction of dementia during 7-years of follow-up.
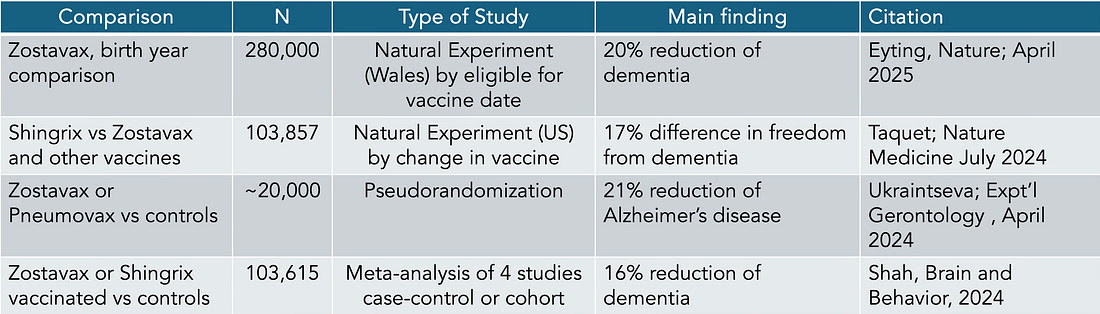
These 2 studies are roughly concordant with the prior studies as summarized in this Table that includes a smaller one with a pseudorandomization algorithm and a meta-analysis of 4 case control or cohort studies.
The new report from Stanford researchers, led by Markus Eyting, Pascal Geldsetzer, and colleagues, was by far the most convincing because of the elegant and systematic analysis that looked at other medical care, use of medications, difference in health care after Shingles, uptake of other vaccinations, effects on other health outcomes, and found no evidence for any differences. They also extended the analysis to combining Wales and England data for confirmation and allude to similar magnitude of benefit in their assessment in multiple other countries.
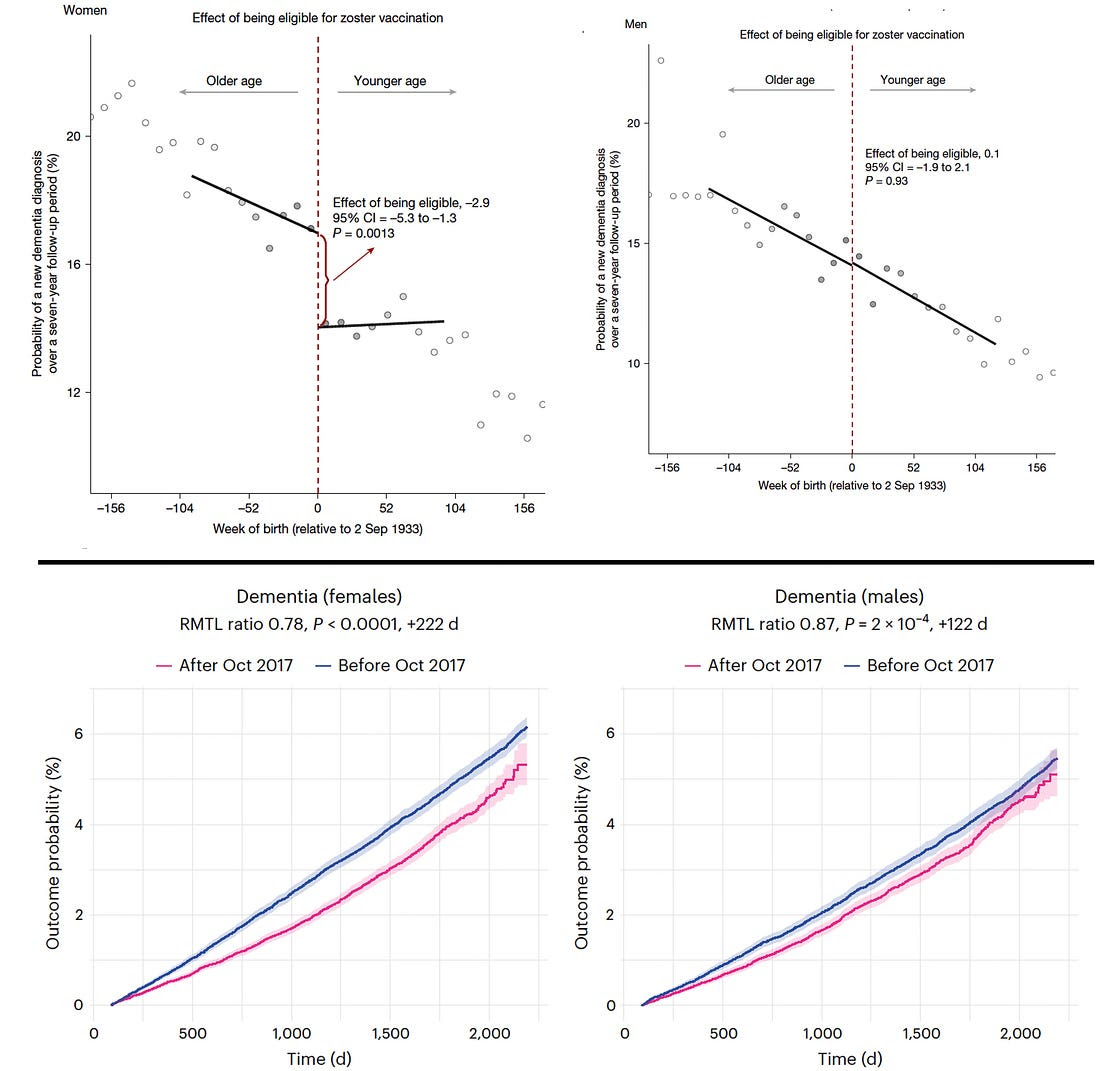
Notably in both of the natural experiments the apparent benefit was largely confined to women (top, new study, bottom Taquet et al, 2024 study). Women are more at risk for developing dementia during older age and there appears to be sex differences in the pathogenesis of dementia and with the immune system responses to vaccines. We’ll come back to this later under mechanism.
But also note one peculiar and interesting finding. Since Shingrix is more effective against the Varicella Zoster Virus (VZV) and in reducing Shingles than Zostavax, why was the benefit similar for Shingrix vs Zostavax compared with Zostavax and no vaccine? That would suggest that if there was a natural experiment for Shingrix vs no vaccine (and there isn’t), the result would be double (or roughly 35-40% reduction of dementia). That would be a very large magnitude of benefit and unlikely. Of course, these two reports used very different populations and analyses, so it is hard to make comparisons between them.
Nevertheless, on the basis of reviewing these data I would conclude there is very likely some protection vs dementia conferred by shingles vaccines. Indeed, Anupam Jena, an expert in natural experiments (he wrote the book Random Acts of Medicine and I interviewed him about that here) wrote the accompanying editorial to the new paper with the quote below:
“…the implications of the study are profound. The vaccine could represent a cost-effective intervention that has public-health benefits strongly exceeding its intended purpose.”—Anupam Jena MD PhD
2. Is this effect for reducing Alzheimer’s disease or dementia?
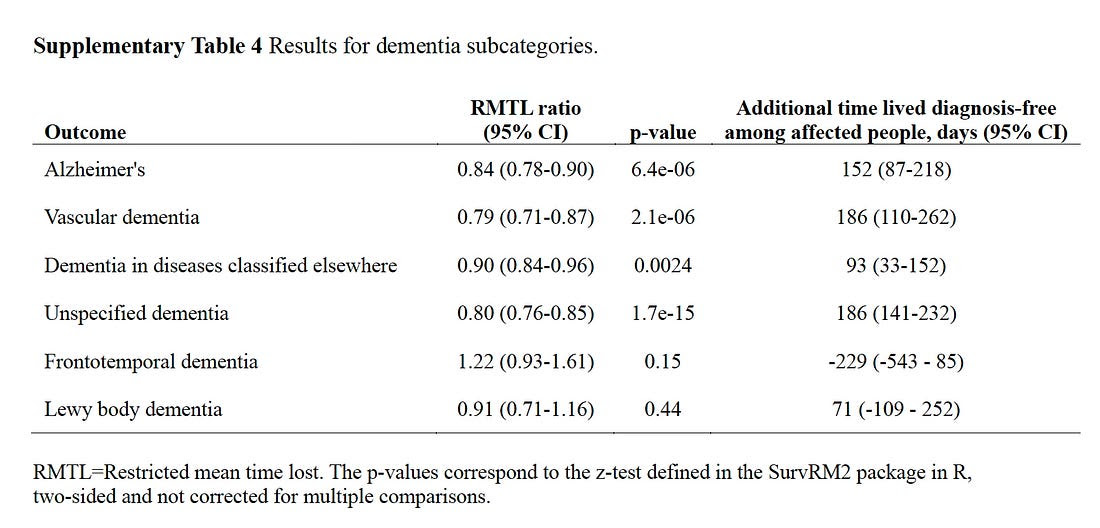
The simple answer is we don’t know. But the question was probed in a couple of these studies. In the Taquet et al natural experiment the benefit was seen for most types of dementia (except Frontotemporal) as seen below.
In the report by Ukraintseva et al, the protective effect was much more for Alzheimer’s disease (21%) than dementia (10%). Unfortunately, the other studies did not shed light on this question. It is a shame that the placebo-controlled trials of Zostavax and Shingrix did not prospectively assess such outcomes. A sharp signal for reducing Alzheimer’s would help with the next question, by partitioning the effect from vascular dementia or other subtypes..
3. What is the mechanism of the benefit?
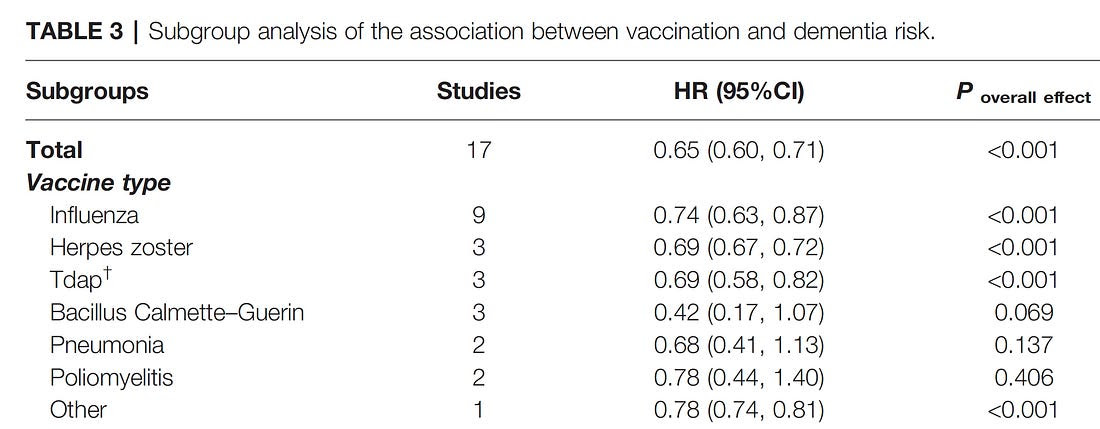
There are many prior studies that have indicated about ~20% or more reduction of dementia with a variety of vaccines including tetanus diphtheria with or without pertussis, pneumococcal vaccine, flu shots, and several others as reviewed here (and the Table below). The effect size (hazard ratio, HR) for many is even more than the natural experiment Herpes Zoster vaccine studies, but all of these are observational, retrospective studies finding association links with multiple confounding factors.
The big question is whether the apparent benefit of reduction of dementia risk in the new study is specific to Herpes Zoster (aka Varicella Zoster Virus, VZV) or is it simply a non-specific effect of revving up the immune response? Here’s a nice video made by the Stanford team about the reactivation of VZV and shingles, with the summary of their study.
To address this question, these authors looked at the effect of multiple bouts of shingles and saw a higher rate of dementia, suggesting that reactivation of the virus increases the risk. And there was less dementia in the individuals who took an antiviral medication for shingles. There is also the intriguing sex difference effect of more prominent dementia reduction in women which may reflect the vaccine’s impact on the immune response. These studies reinforce the potential link between VZV and dementia, but the overall evidence is much softer than we have seen for the Epstein-Barr virus (EBV) and multiple sclerosis. There’s a prerequisite of EBV exposure to develop MS, although other factors contribute, such as genetics. Nothing like that has yet been clearly established for VZV and dementia.
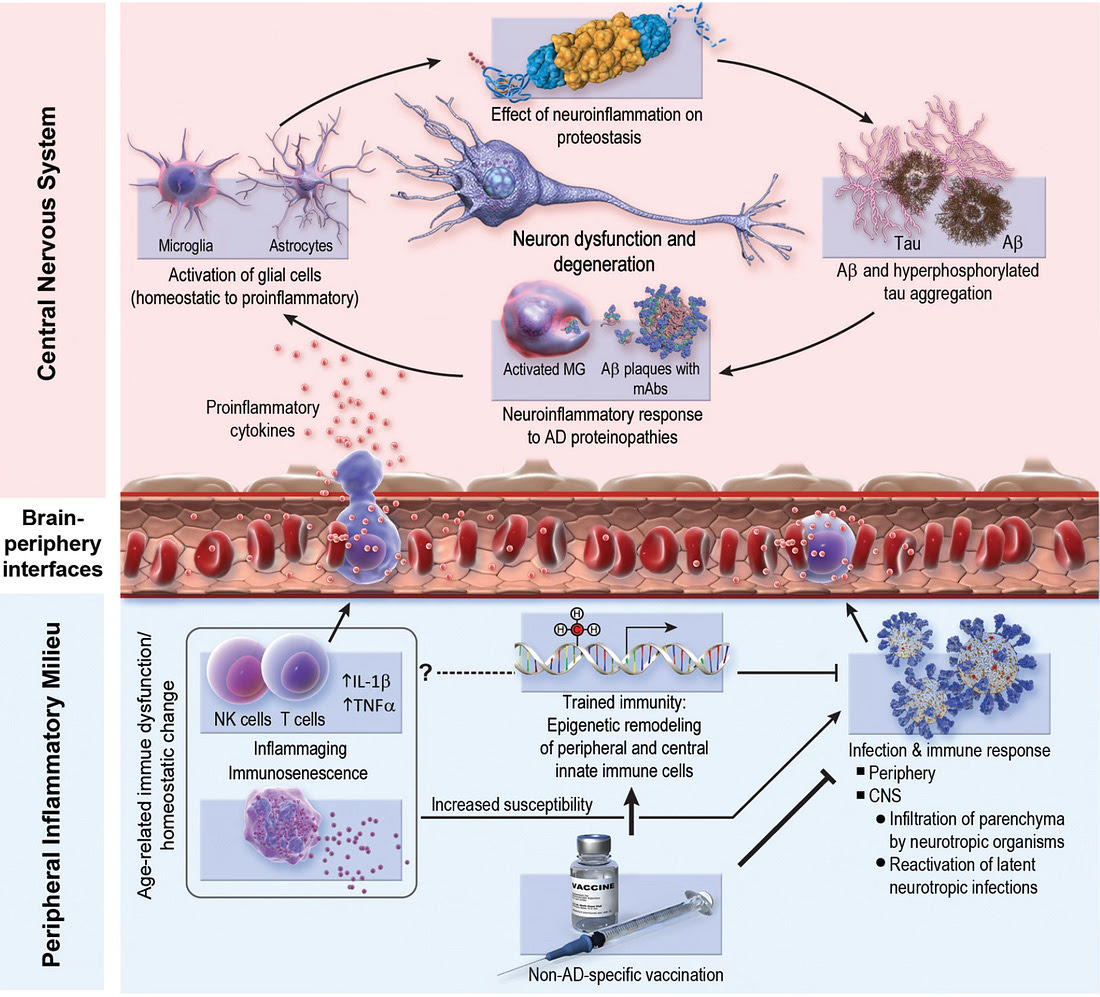
The non-specific effects of vaccination cannot be ruled out. This refers to revving up the peripheral immune response that is seen with aging (“immunosenescence”) in the lower panel, and the interface with the inflammation that can be blunted or provoked in the brain.
Concluding Remarks
The new study is impressive and the best yet to show an effect of an outdated live-attenuated Shingles vaccine on reduction of dementia during extended follow-up. It does not, however, prove the effect is Herpes Zoster specific, a long lingering question concerning the virus’s possible underpinning role for Alzheimer’s disease, no less dementia in general. The sex differences for the two natural experiments are striking for predominance of benefit in women, which can be used to either support the vaccine specific effect or further question what explains such marked differences.
One of the important takeaways from this review is the importance of natural experiments which in some ways are better than randomized trials. The latter require fulfilling entry criteria so the enrolled participants are only a subset of those screened. In contrast, the natural experiment doesn’t introduce such selection bias. When they are available and analyzed properly, they are a gift for medical research. Unfortunately, there aren’t many of them like the current study to help us out.
My personal take on Shingrix was affected by the Taquet report in 2024 which I included in my new book Super Agers which highlights the influence of the immune system for healthspan. I had been reluctant to get the Shingrix vaccine despite the urging of my internist. That was because many of my colleagues had severe acute reactions, feeling very sick with a flu-like illness for a couple of days. I had already experienced that with Covid shots and wasn’t looking to go through it again.
But last fall I had the 2 doses of Shingrix (two months apart) with minimal side effects. That was not only because I don’t ever want to get shingles (BTW, I hate the TV commercials for Shingrix “Shingles Doesn’t Care” which are a real scare tactic and turn off) but also the added potential protection against dementia. Since last year we now have even more data to support getting the vaccine, a twofer. We still need to get answers to many unsettled questions that I’ve reviewed here, but it seems increasingly likely there’s a bonus benefit.
Source GROUNDTRUTHS

Leave a Reply